Atrial Septal Defect
Quick Facts
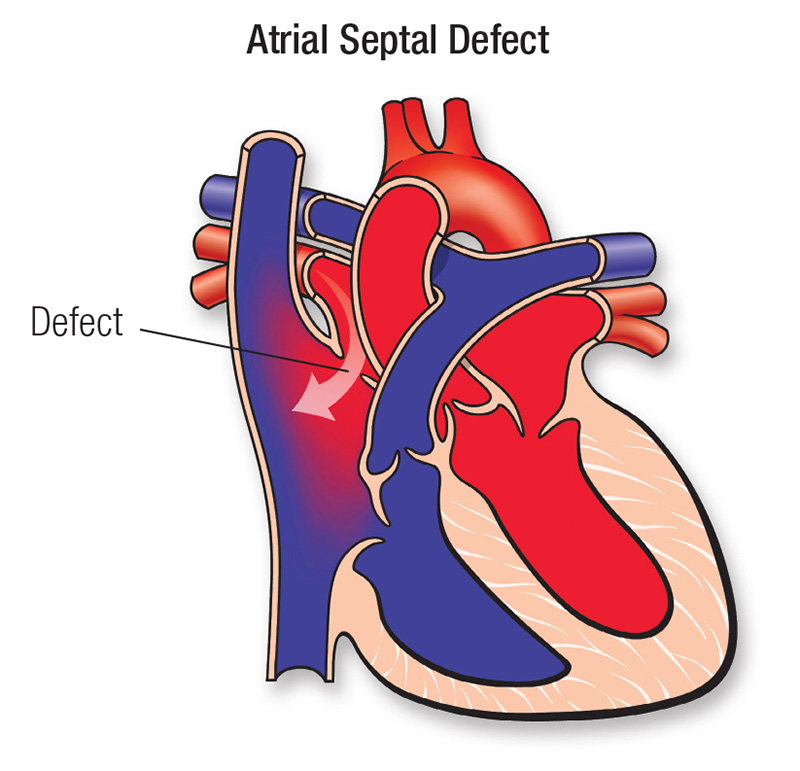
- An atrial septal defect (ASD) is a hole in the wall that separates the upper chambers of the heart.
- If the ASD is large, it can make the heart and lungs work harder. This can damage the arteries in the lungs.
- Small openings may not need to be repaired. Large openings can be repaired with surgery.
What is an atrial septal defect?
An atrial septal defect (ASD) is a hole in the wall that separates the upper chambers of the heart. This opening allows oxygen-rich blood from the left atrium to flow into the right atrium, where oxygen-poor blood is normally found. As a result, extra blood flows to the right side of the heart and to the lungs.
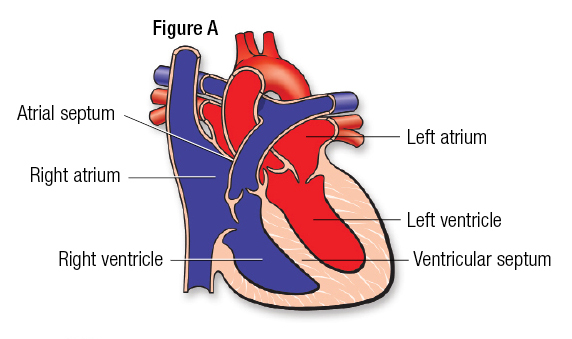
The heart has four chambers. The upper two chambers are the atria, and the lower two are the ventricles (Figure A). The chambers are separated by a wall of tissue called the septum. Blood is pumped through the chambers, aided by four heart valves. The valves open and close to let the blood flow in only one direction.
What causes an atrial septal defect?
Every child is born with a normal opening between the upper heart chambers called the foramen ovale. This allows blood to bypass the lungs before birth, when the lungs are not yet used for oxygen exchange. After birth, the opening is no longer needed as the lungs expand and are used. This opening usually closes or becomes very small within several weeks or months.
Sometimes the opening is larger than normal and doesn’t close after birth. In most children, the cause is unknown. Genetic factors can sometimes play a role. Some children can have other heart defects along with ASD.
How does an ASD affect the heart?
Normally, the left side of the heart pumps blood only to the body, and the right side of the heart pumps blood only to the lungs. In a child with ASD, blood can travel across the hole from the left upper heart chamber (left atrium) to the right upper chamber (right atrium) and out into the lung arteries.
If the ASD is large, the extra blood being pumped into the lung arteries makes the heart and lungs work harder. The arteries in the lung can gradually become damaged, sometimes leading to pulmonary hypertension.
If the hole is small, it may not cause symptoms or problems. Many healthy adults still have a small opening in the wall between the atria, sometimes called a patent foramen ovale (PFO). It usually does not cause problems.
What symptoms can an ASD cause?
Many people with ASD have no symptoms. When the opening is small, symptoms typically don’t occur because the heart and lungs don’t have to work harder than normal. Larger openings may cause mild shortness of breath, especially during physical activity. On examination, the only abnormal finding may be a heart murmur (sound heard with a stethoscope) or other unusual heart sounds.
Over time, if increased blood flow leads to damage in the lung blood vessels, pressure in the lungs can rise. This can result in more limitations and, in rare cases, progression to Eisenmenger syndrome.
Can an atrial septal defect be repaired?
If the opening is small, surgery and other treatments may not be needed. Small ASDs that are discovered in infants often close or narrow on their own. There is no medication that will make the ASD get smaller or close faster than it would naturally.
If the ASD is large, it can be closed with open-heart surgery or by cardiac catheterization using a device that seals the opening. In some cases, such as when the defect is in an unusual location or when other heart defects are present, catheter closure is not possible and surgery is needed.
Closing a large ASD by open-heart surgery is usually done in early childhood, even in patients with few symptoms, to prevent future complications.

ASD in children: What families need to know
How does an ASD affect my child?
Children with an ASD often have no symptoms. If the opening is small, it won’t cause symptoms because there is not much extra blood flow to the lungs. In children with a large ASD, the main risk is to the blood vessels in the lungs because more blood than normal is being pumped there. Over time, usually many years, this may cause damage to the lung blood vessels.
Which activities can my child do?
Your child may not need special precautions and may be able to take part in normal activities without increased risk. After surgery or catheter closure, your child’s pediatric cardiologist may advise some activity changes for a short time. After successful healing from surgery or catheter closure, no restrictions are usually needed.
What will my child need in the future?
For a short time after surgery to close an ASD, a pediatric cardiologist must regularly examine the child. Sometimes medications to prevent blood clots and infection are used for a few months after ASD closure. Depending on the type of ASD, your pediatric cardiologist may examine your child periodically to watch for uncommon problems.
The long-term outlook is excellent, and usually no medications, additional surgery or catheterization are needed.
How can endocarditis be prevented?
Most children with an ASD are not at increased risk of developing endocarditis, an infection in the heart. Your child’s cardiologist may recommend antibiotics before certain dental procedures for a period of time after ASD repair.
ASD in adults: What to expect
What can an adult expect after childhood ASD surgery?
A large ASD is usually closed in early childhood, even in patients with few symptoms, to prevent future complications. Some defects are closed with a patch of pericardium (the normal lining outside the heart) or a synthetic material. However, many defects that required surgery may have been sewn closed without using a patch. The prognosis after ASD closure during childhood is excellent. Late complications are uncommon.
If the defect persists, should it be repaired in adulthood?
If the opening is small, surgery or other treatment may not be needed.
Most large atrial septal defects can be closed with open-heart surgery or through cardiac catheterization using a device to seal the opening. This is called interventional or therapeutic catheterization. In some cases, such as when the defect is in an unusual location or when other heart defects are present, catheter closure is not possible and surgery is needed. Even when the defect is diagnosed in adulthood, closure of large defects is beneficial.
Possible Complications with an ASD
Adults with small unrepaired or repaired ASDs rarely have late complications. Those who have symptoms such as palpitations or fainting should be evaluated by a cardiologist and may need medication.
When an ASD is diagnosed late in life, heart function may be affected. In some cases, the person can develop heart failure and, rarely, pulmonary hypertension.
Patients who have had a transient ischemic attack (TIA) or a stroke and are found to have a PFO may be treated with aspirin or another antiplatelet medication. If another stroke occurs despite medication, closure of the PFO or ASD may be needed. Most people with small PFOs and ASDs do not have strokes and do not need their defects closed.
Ongoing Care
Patients with a history of ASD should be seen periodically by a cardiologist to watch for uncommon problems. For a short time after surgery to close an ASD, a cardiologist must regularly examine you. The long-term outlook is excellent, and usually no medications, additional surgery or catheterization are needed.
Medical Follow-up
After ASD closure, some patients may take medications to prevent blood clots or infection. It is uncommon to need medication beyond six months.
A cardiologist may monitor your recovery using noninvasive tests if needed. These include:
These tests will help show if more procedures, such as a cardiac catheterization, are needed.
Activity Restrictions
Most patients with small, unrepaired ASDs or repaired ASDs do not need to take special precautions. They can usually participate in normal activities without increased risk.
After recent surgery or catheter closure, a cardiologist may recommend temporary limits on physical activity, even if pulmonary hypertension is not present. Once healing is complete, activity restrictions are usually not needed. An exception applies to patients who have developed high pressure in the lungs (pulmonary hypertension; see Eisenmenger syndrome). They should refrain from high-intensity sports.
Endocarditis Prevention
Steps to prevent endocarditis aren’t needed beyond six months after the repair, either by surgery or device.
Pregnancy
Once an ASD is closed and no opening remains, the risk associated with pregnancy is very low. Pregnancy-related risk is higher when an ASD is unrepaired, but pregnancy is usually safe unless pulmonary hypertension is present.
A large unrepaired ASD may lead to heart failure during pregnancy. However, this is often well controlled with medication when found early. There is also a small risk of stroke during pregnancy, so precautions to reduce risk of blood clot may be recommended.
Will another surgery be needed?
Once an ASD is closed, it’s unlikely that more surgery will be needed. In rare cases, a small opening will remain. The size of the remaining opening will determine if more treatment is needed.





